Lower limb · Calf — muscular · Elite level
Soleus Muscle Injury — High Performance Football
Criteria-based rehabilitation stratified by BAMIC anatomical site. Knee-flexed loading is mandatory; sprint exposure must be completed before return-to-training. Built around Pedret (2015) prognosis data and Lai (2014) sprint biomechanics.
Why the soleus matters in football
The soleus is the primary ankle work generator in stance-phase locomotion, responsible for roughly 53–74% of ankle positive work via elastic Achilles tendon recoil across speeds of 2–8 m/s (Lai 2014). Its monoarticular architecture, type-I fibre dominance (60–90%), and coupling to the long Achilles tendon define both its central role in running and its specific injury vulnerability.
Soleus injuries in footballers are dominated by cumulative load mechanisms, not single-event explosive tears. They concentrate at five anatomical sites — and the prognosis varies dramatically depending on which one.
Prognosis by anatomical site (Pedret 2015, n=44)
| Site | Location | BAMIC suffix | Mean RTP | CIT involved |
|---|---|---|---|---|
| MTL | Proximal lateral myotendinous junction | b | ~19 days | No |
| MTM | Proximal medial myotendinous junction | b | ~25 days | No |
| MFA | Myofascial anterior | a | ~33 days | No |
| MFP | Myofascial posterior | a | ~38 days | No |
| MTC | Central intramuscular tendon (CIT) | c | ~44 days | Yes — worst prognosis |
MTC mean RTP 44.3 ± 23.0 days. CIT injuries follow tendon-grade healing timelines and progress at 1.5–2× slower rate than MTJ injuries.
Two cardinal principles
- Knee-flexed loading is mandatory. With the knee at 30–90°, the gastrocnemii shorten and lose force capacity, making the soleus the primary plantarflexor. Any protocol omitting bent-knee loading under-doses the soleus.
- Sprint exposure must be completed before return-to-training. Elastic energy contribution to ankle work rises from 53% (2 m/s) to 74% (8 m/s). Without sprint re-exposure, the storage-release mechanism is undertrained and re-injury risk concentrates exactly where the football demand sits.
Loading hierarchy
- Isometric: 45 s holds at 70% MVC — tendon stiffness stimulus, cortical analgesia (Rio protocol), reduced neuromotor inhibition. Allows early loading without tissue stress concentration.
- Isotonic (concentric/eccentric): reintroduce dynamic ankle work at sub-maximal loads.
- Heavy Slow Resistance (HSR): 65–90% 1RM, 3+3 s tempo, knee-flexed emphasis. Gold standard for tendon remodelling — induces collagen type-I synthesis, improves MTU stiffness, restores force-generating capacity.
- Plyometric: restore the elastic energy storage-release mechanism essential for football running.
- Sprint: graded sprint re-exposure before RTT clearance.
CIT/MTC injuries require an extended HSR phase (minimum 2 additional weeks) before plyometrics or running re-exposure.
Why this matters: RFD over peak force
The Rate of Force Development (RFD) — not peak force alone — governs functional capacity at sprint contact times (~100 ms). Late-phase rehabilitation must include explosive intent and stretch-shortening-cycle (SSC) based exercises. A soleus that tests strong on slow isokinetic but lacks RFD will fail the first true sprint exposure.
Who this protocol is for
- Sports physiotherapists managing soleus injuries in football and high-performance running.
- Medical departments standardizing calf-injury workflows around BAMIC and CIT involvement.
- Strength & conditioning coaches responsible for late-stage reconditioning and sprint re-exposure.
- Clinicians who want a worked example of criteria-based — not calendar-based — return-to-play decision-making.
Download the full protocol (PDF)
Includes the complete phase-by-phase prescription, criteria for transition, sprint re-exposure ladder, and CIT-adjustments. Free for qualified health and performance professionals.
Frequently asked questions
Why is knee-flexed loading mandatory for soleus rehabilitation?
With the knee at 30–90°, the gastrocnemii shorten and lose force capacity, making the soleus the primary plantarflexor. Any protocol omitting bent-knee loading under-doses the soleus and leaves a strength gap that re-emerges under sprint demand.
What is BAMIC and why does it matter for prognosis?
BAMIC (British Athletics Muscle Injury Classification) classifies muscle injuries by anatomical site as "a" (myofascial), "b" (myotendinous junction) and "c" (tendon-associated). For the soleus, central intramuscular tendon (CIT/MTC) injuries (BAMIC-c) carry the worst prognosis — mean RTP ~44 days vs ~19–25 days for MTJ injuries (Pedret 2015).
Why is sprint exposure required before return-to-training?
Elastic energy contribution to ankle work increases from 53% (2 m/s) to 74% (8 m/s) (Lai 2014). Without sprint re-exposure, the storage-release mechanism is undertrained and the athlete is exposed to re-injury when football demands suddenly bring them above their reconditioned ceiling.
What is the loading hierarchy?
Isometric → Isotonic (concentric/eccentric) → Heavy Slow Resistance → Plyometric → Sprint. Each tier builds on the previous one. Isometrics provide tendon stiffness stimulus and cortical analgesia; HSR (65–90% 1RM, 3+3 s tempo, knee-flexed emphasis) is the gold standard for tendon remodelling. CIT/MTC injuries require an extended HSR phase (minimum 2 additional weeks) before plyometrics or running.
Related protocols
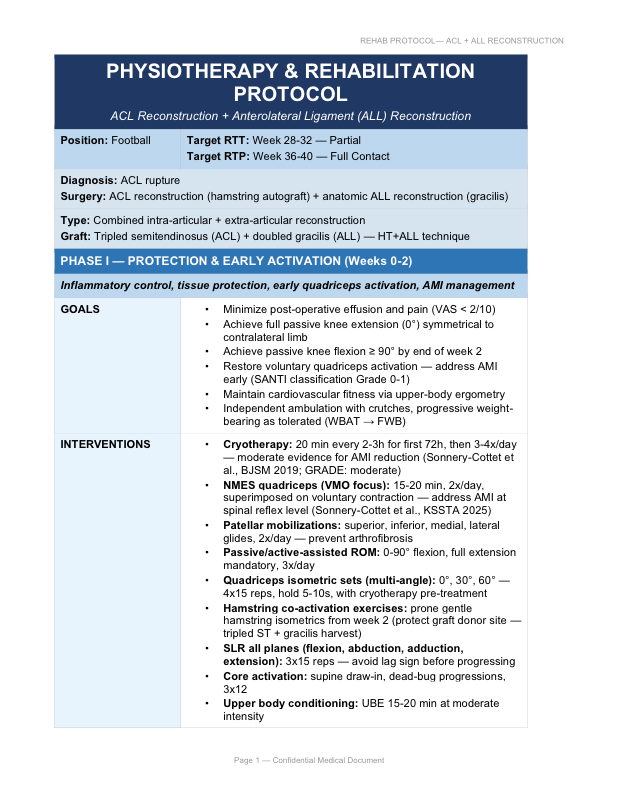
ACL + ALL Reconstruction
Phased rehabilitation for combined ACL + Anterolateral Ligament reconstruction.
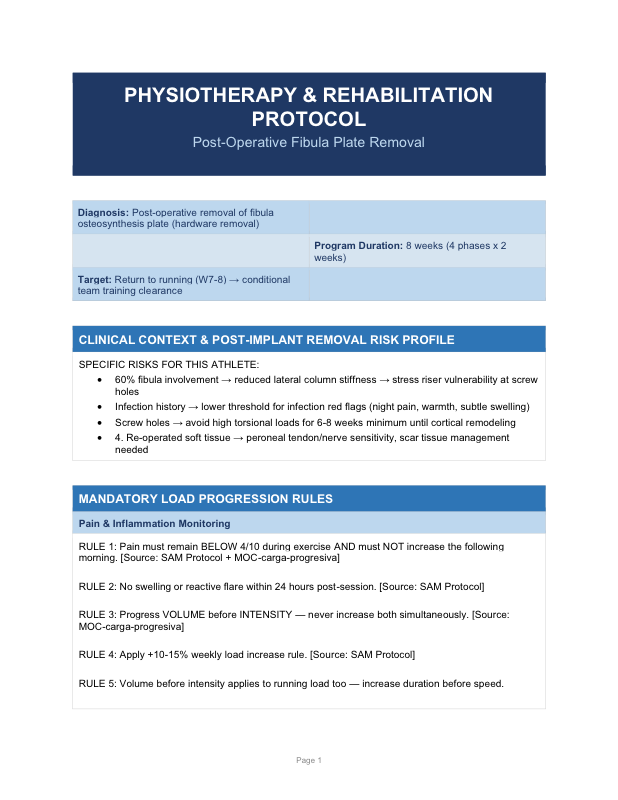
Post-Operative Fibula Plate Removal
Eight-week rehabilitation in 4 phases of 2 weeks. Return to running W7–8.