Lower limb · Knee — surgical · Elite level
ACL + Anterolateral Ligament (ALL) Reconstruction
A criteria-based rehabilitation protocol for combined ACL + ALL reconstruction with hamstring autograft and gracilis, designed for professional football. Targets Return-To-Training at week 28–32 and Return-To-Play at week 36–40.
Overview
This protocol governs the rehabilitation of an athlete after combined intra-articular ACL reconstruction and extra-articular anatomic ALL reconstruction. The dual procedure addresses both anteroposterior translational instability (ACL) and anterolateral rotational laxity (ALL), and has been shown to reduce secondary graft-rupture rates in young pivoting athletes compared with isolated ACL reconstruction.
Progression is governed by objective criteria, not calendar dates. Time windows are clinical guides — every phase transition requires the athlete to satisfy strength, ROM, swelling, and functional testing thresholds before advancing.
Protocol structure
The program is organized in five progressive phases, each with explicit goals, interventions, and progression criteria.
-
Phase I — Protection & early activation (weeks 0–2)
Inflammatory control, tissue protection, and early quadriceps activation. AMI is addressed at the spinal reflex level via cryotherapy and NMES superimposed on voluntary contraction. Mandatory full passive extension symmetrical to the contralateral limb. Patellar mobilizations prevent arthrofibrosis. Hamstring isometrics are reintroduced cautiously from week 2 to protect the donor site.
-
Phase II — Early mobility & transition (weeks 2–6)
Gait normalization without crutches, full ROM (0–120°+), early closed-kinetic-chain loading, and proprioceptive training. Aerobic conditioning maintained via stationary bike and pool when available.
-
Phase III — Strength & neuromuscular control (weeks 6–14)
Bilateral and unilateral strengthening at progressive intensity. Quadriceps and hamstring strength symmetry targets above 70% LSI. Introduction of low-intensity running on alter-G or treadmill once criteria are met.
-
Phase IV — Power, plyometrics & sport-specific (weeks 14–28)
Heavy slow resistance for tendon and graft conditioning, progressive plyometrics (bilateral → unilateral), change-of-direction drills, and on-field reintroduction. Strength symmetry target ≥90% LSI before plyometric progression.
-
Phase V — Return-to-Training & Return-to-Play (weeks 28–40)
Full football-specific conditioning, contact reintroduction, position-specific drills, and progressive integration into team training. Final RTP clearance gated by hop test battery, isokinetic testing, on-field exposure, and psychological readiness (ACL-RSI).
Evidence base
The protocol integrates the contemporary literature on combined ACL + ALL reconstruction and AMI management:
- Sonnery-Cottet et al., AJSM 2017 — reduced graft rupture rates in combined ACL + ALL.
- Sonnery-Cottet et al., BJSM 2019 — cryotherapy and AMI reduction.
- Sonnery-Cottet et al., KSSTA 2025 — SANTI classification of AMI severity.
- Loading hierarchy informed by progressive overload principles validated in tendinopathy and post-surgical knee literature.
Who this protocol is for
- Sports physiotherapists working in professional or semi-professional football.
- Medical departments standardizing ACL + ALL postoperative care.
- Orthopedic surgeons coordinating rehabilitation handover with their physiotherapy team.
- Strength & conditioning coaches in elite sports environments needing aligned reconditioning timelines.
Download the full protocol (PDF)
The complete protocol contains every phase with detailed exercise prescription, progression criteria, and red-flag rules. Free for qualified health and performance professionals.
Frequently asked questions
Why combine ACL and ALL reconstruction?
Adding an anatomic ALL reconstruction to an ACL graft significantly reduces the rate of secondary ACL graft rupture in young pivoting athletes (Sonnery-Cottet et al., AJSM 2017). The ALL controls anterolateral rotational laxity that an isolated ACL graft cannot fully restrain, especially in football.
When can a footballer return to play after ACL + ALL reconstruction?
This protocol targets Return-To-Training (partial, non-contact) at week 28–32 and Return-To-Play (full contact, competitive) at week 36–40. Progression is criteria-driven, not calendar-driven — strength symmetry, hop tests, on-field exposure, and psychological readiness all gate the next phase.
What is AMI and why is it managed so early?
AMI (Arthrogenic Muscle Inhibition) is the spinal-reflex shutdown of quadriceps activation following knee injury and surgery. Left untreated it stalls strength recovery for months. The SANTI classification (Sonnery-Cottet et al., KSSTA 2025) grades AMI severity and guides early NMES + voluntary contraction superimposition starting week 1.
Can I use this protocol for an isolated ACL reconstruction?
The general phase logic transfers, but the timeline and graft-protection cues are tuned for the combined ACL + ALL technique with hamstring autograft + gracilis. Isolated ACL reconstructions with BTB or quadriceps tendon grafts have different early-phase considerations and should follow graft-specific protocols.
Related protocols
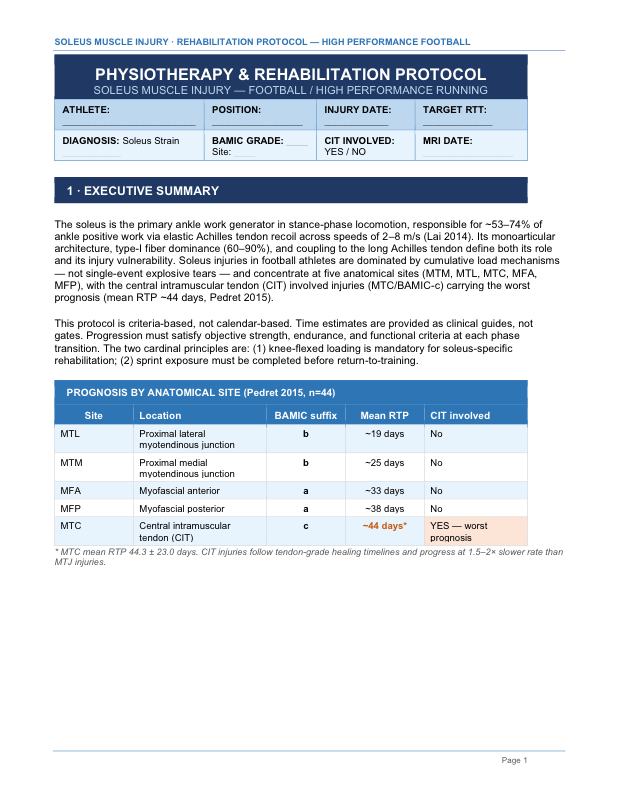
Soleus Muscle Injury — High Performance Football
Criteria-based rehabilitation stratified by BAMIC site (MTM, MTL, MTC, MFA, MFP).
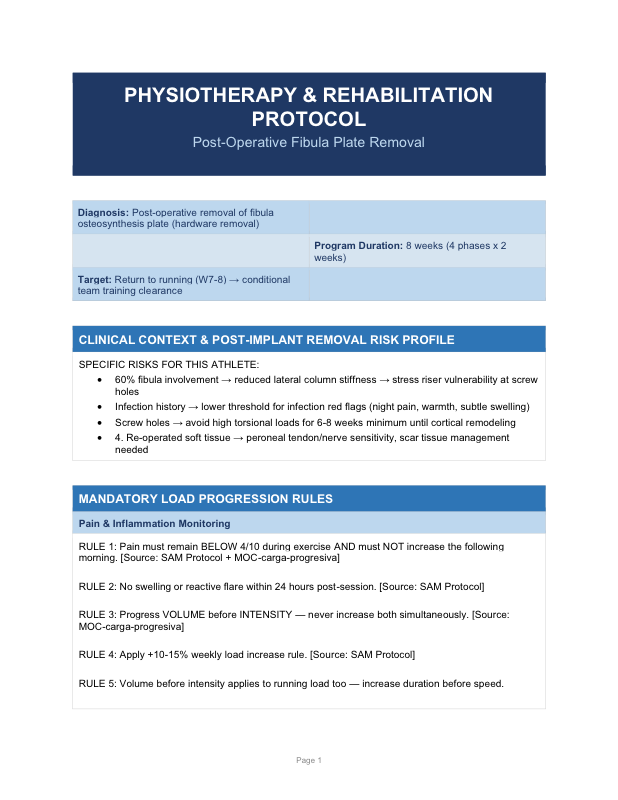
Post-Operative Fibula Plate Removal
Eight-week rehabilitation in 4 phases of 2 weeks. Return to running W7–8.