Lower limb · Ankle — post-op · Elite level
Post-Operative Fibula Plate Removal
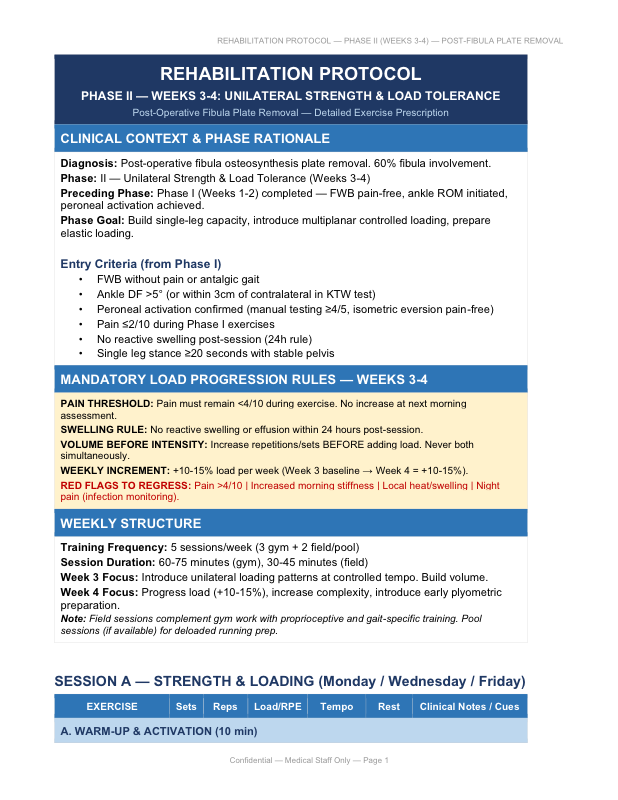
An eight-week, four-phase rehabilitation protocol for athletes following fibula osteosynthesis plate removal. Built around explicit load progression rules and infection-specific monitoring, with return-to-running targeted at weeks 7–8.
Clinical context
Hardware removal after fibula osteosynthesis is a deceptively complex rehabilitation case. The bone is no longer instrumented, but each screw hole creates a cortical defect that acts as a stress riser, and re-operated soft tissue (peroneal tendons, scar tissue) requires careful reintroduction of load. With 60% fibula involvement and a prior infection history, the threshold for caution is lower than in a routine post-fixation case.
Mandatory load progression rules
Every progression in this protocol is governed by five non-negotiable rules:
- Pain threshold: pain must remain <4/10 during exercise and not increase the following morning.
- Swelling rule: no swelling or reactive flare within 24 hours post-session.
- Volume before intensity: progress repetitions or sets before adding load — never both simultaneously.
- Weekly increment: +10–15% load per week, not more.
- Running-load rule: volume before intensity applies to running too — duration before speed.
Red flags for regression
- Pain >4/10 during exercise → reduce load 30%, reassess in 48 h.
- Increased morning stiffness vs. baseline → reduce volume, increase mobility work.
- Local warmth or swelling → stop loading for 24–48 h.
- Night pain at the surgical site → stop all loading, urgent medical review (earliest indicator of infection).
- Fatigue-related pain at screw-hole sites → reduce impact activities, reassess bone integrity.
Phase structure
-
Phase I — Recovery & activation (weeks 1–2)
Wound care, FWB pain-free gait, ankle ROM initiation, peroneal activation, single-leg stance baseline.
-
Phase II — Unilateral strength & load tolerance (weeks 3–4)
Build single-leg capacity, multiplanar controlled loading, prepare for elastic loading. Detailed exercise prescription for this phase →
-
Phase III — Elastic loading & running prep (weeks 5–6)
Progressive plyometric introduction, running mechanics drills, pool-deloaded running if available, controlled change-of-direction at sub-maximal intensity.
-
Phase IV — Return to running & conditional clearance (weeks 7–8)
Linear running progression (volume → intensity → speed), reintroduction of football-specific actions, conditional clearance for team-training integration once criteria are satisfied.
Biomechanical precautions
With 60% fibula involvement, lateral column stiffness is reduced. Cortical bone needs 6–12 weeks to remodel screw-hole defects. The peroneal musculature may be sensitized from re-operation. If syndesmotic screws were part of the original fixation, syndesmotic stability should be reassessed post-removal.
Strictly prohibited in early phases (weeks 1–4): high-speed cutting or change of direction, maximal jumping, contact training, single-leg landings from height.
Who this protocol is for
- Sports physiotherapists managing post-hardware-removal cases in football.
- Medical departments standardizing post-operative ankle rehabilitation.
- Clinics handling complex re-operation cases with prior infection history.
Download the full protocol (PDF)
The complete protocol contains every phase with exercise prescription, progression criteria, and red-flag rules. Free for qualified health and performance professionals.
Frequently asked questions
Why is the bone weaker after plate removal?
Each removed screw leaves a cortical defect (a "screw hole") that acts as a stress riser. Cortical bone requires 6–12 weeks to remodel these defects, and high torsional loads should be avoided during that window. With 60% fibula involvement, lateral column stiffness is meaningfully reduced until remodelling completes.
When can the athlete start running again?
The protocol targets return to running between weeks 7 and 8, conditional on satisfying the load-tolerance and pain criteria of phases I–III. Volume is progressed before intensity — duration before speed. Conditional team-training clearance follows once running is consolidated.
What red flags should regress or stop loading?
Pain >4/10 during exercise (reduce load 30%), increased morning stiffness vs. baseline, local warmth or swelling (stop loading 24–48 h), and night pain at the surgical site (stop all loading and seek medical review immediately — earliest indicator of infection). With prior infection history, the threshold to escalate is lower.
Why no high-speed cutting in early phases?
Cutting and sudden change of direction generate high torsional loads through the lateral column. Until cortical remodelling of the screw holes is complete (6–8 weeks minimum), these movements concentrate stress at the holes and risk re-fracture.
Related protocols
Fibula Plate Removal — Phase II (Weeks 3–4)
Detailed exercise prescription for the unilateral strength and load tolerance phase.
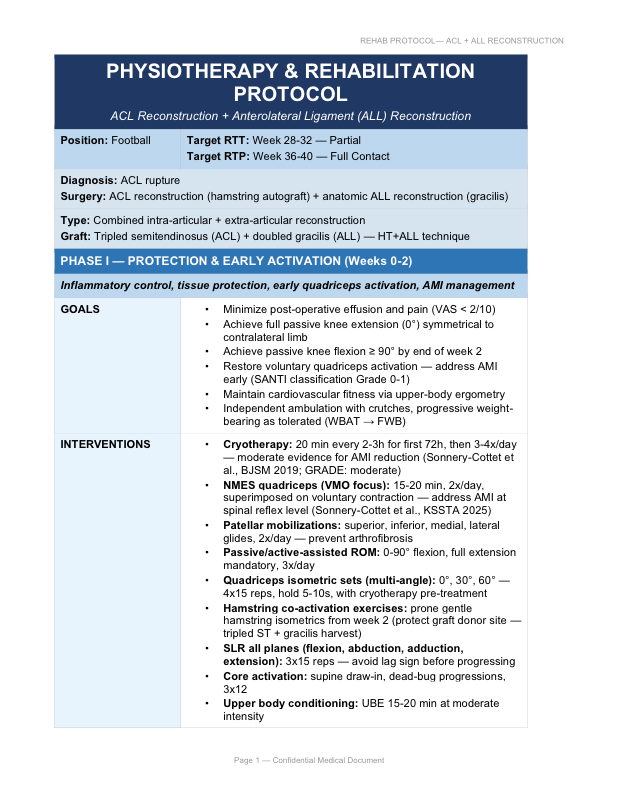
ACL + ALL Reconstruction
Phased rehabilitation for combined ACL + Anterolateral Ligament reconstruction. RTP W36–40.